Skincare active combinations. What to mix, what not to mix.


My personal story with stacking actives
I want to start this post with a story, because it is the reason I am writing it.
A few months ago a friend of mine showed up looking miserable. Her cheeks were red, her skin was tight, she had little flaky patches around her nose, and there was that specific kind of stinging that makes you afraid to touch your own face. She told me she had recently gotten really into skincare. She had ordered a bunch of products from The Ordinary, watched a stack of TikToks, and started experimenting.
So I asked her the only question that matters in these moments: what exactly did you put on your face?
She listed it off. A vitamin C serum. A retinol product. A glycolic acid toner "a few times a week." A niacinamide. And, on most days, all of them at the same time because she was trying to "get the most out of the routine."
Two of those, layered together, were the real problem: retinol and L-ascorbic acid (pure vitamin C). She had been applying her retinol on top of her vitamin C serum some evenings, thinking that more actives meant more benefits.
Here is the thing she had completely missed, and that almost everybody misses when they start playing with actives: multiple ingredients can target the same skin goal. Retinol is brilliant against early signs of ageing AND against acne. Vitamin C also fights ageing (through collagen synthesis) AND fades acne scars. So in her head, she was treating "different things." In reality, she was hammering the same biological pathways from two angles, at the same time, with two ingredients that fundamentally do not like each other's pH.
I want to avoid as many people getting stuck in the same situation. So let's break down which actives clash, which ones are quietly fine despite the internet drama, and which combinations are actually smart for specific skin goals.
Why combination mistakes happen: It's about the goal, not the ingredient
Most people think about skincare ingredient by ingredient. "I am using retinol." "I am using vitamin C." "I am using a glycolic toner." But your skin does not experience them as separate items. It experiences them as a combined biological signal.
The real reason people accidentally over-do their routines is that several actives address the same concern through different mechanisms. So you assume you are stacking complementary tools, when in fact you are stacking redundant (and sometimes incompatible) ones.
Here is a quick map of what the most popular actives actually do, sorted by skin goal:
Look at how many actives sit in the "anti-ageing" column. Or in "acne." That is exactly why people accidentally combine retinol with vitamin C (both target ageing) or BHA with benzoyl peroxide (both target acne).
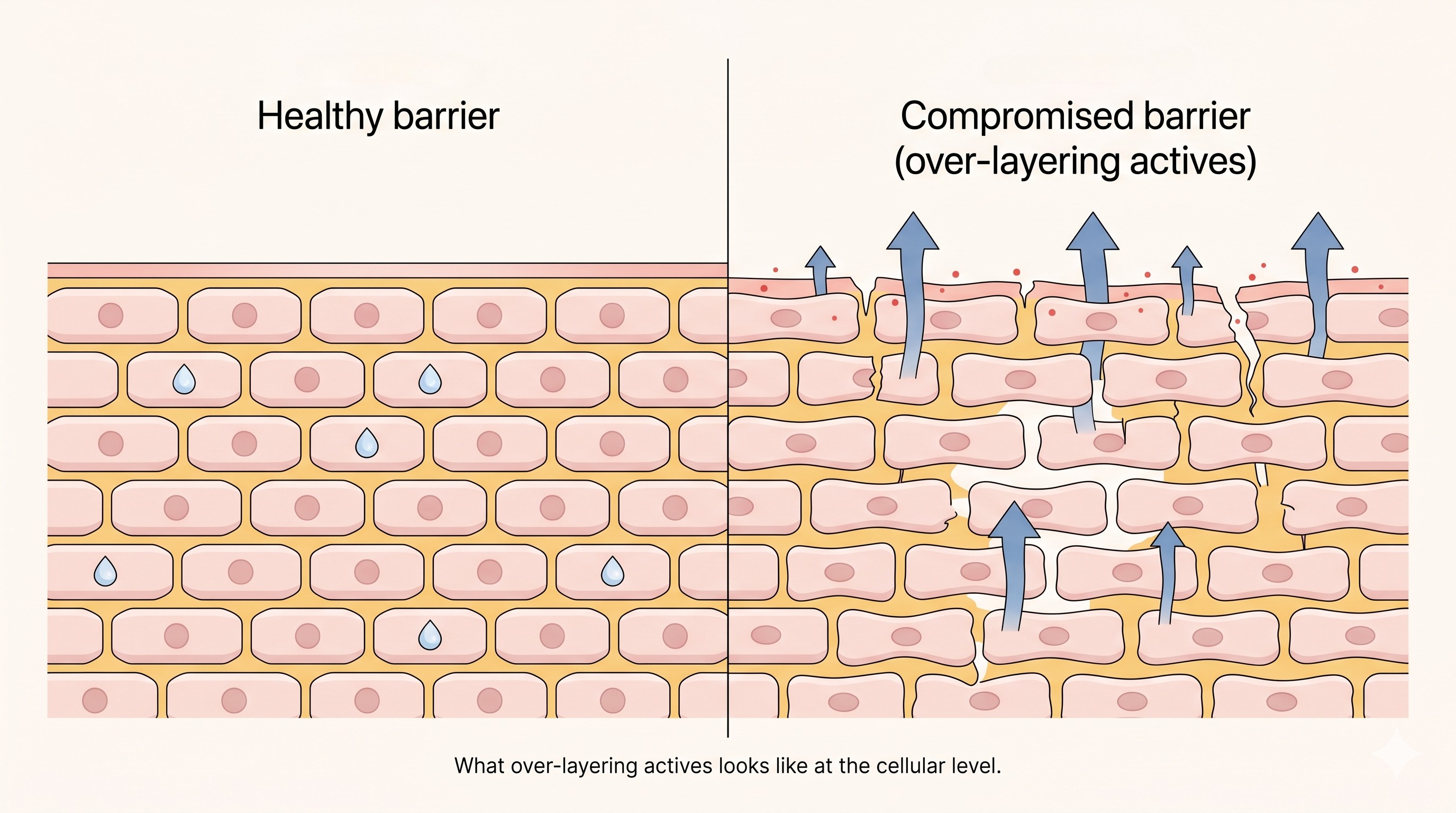
The barrier is the part nobody warns you about. Once it is compromised (which happens easily when you stack actives), every product you put on your face stings, your skin becomes more reactive, and ironically you start losing more water and producing MORE oil, more redness, sometimes more breakouts. The very things you were trying to fix.
The combinations you should NOT stack
Let's start with the ones to actively avoid. Below is a quick-reference table. The deep-dive science follows underneath.
1. Retinol + vitamin C(the classic mistake)
This is the one my friend got wrong, and it is by far the most common stacking mistake among people who get into actives. The reason is purely about overlapping skin goals: both ingredients are amazing for early signs of ageing. Retinol increases cell turnover and stimulates collagen production through its conversion to retinoic acid, which binds to nuclear retinoic acid receptors and modulates gene expression for collagen and matrix proteins (Mukherjee et al., 2006). L-ascorbic acid is the cofactor for prolyl and lysyl hydroxylase, the enzymes that stabilise the collagen triple helix, and it is a potent antioxidant on top (Pullar et al., 2017). So in your head: "I am hitting collagen from two angles, brilliant."
In reality, the formulation chemistry does not cooperate. Vitamin C, specifically, L-ascorbic acid needs a formulation pH below 3.5 to be stable and to penetrate the skin. Most retinoids work optimally at a higher pH (around 5.5-6). When you layer them, you both blunt the activity of one or both ingredients AND pile irritation on irritation. The classical Fitzpatrick & Rostan study confirmed that combining ascorbic acid with tretinoin in a single regimen requires careful timing to manage irritation while preserving photoprotection (Fitzpatrick & Rostan, 2002).
Practical solution: vitamin C in the morning (where its antioxidant activity also boosts your sunscreen's photoprotective effect), retinoid in the evening. You get all the benefits, none of the chaos. If you are using a vitamin C derivative (like ethyl ascorbic acid) instead of pure LAA, the pH conflict largely disappears, but the irritation overlap is still worth being thoughtful about. More about this on my article on vitamin C.
2. Retinol + AHAs / BHAs (anti-ageing on top of anti-ageing)
Retinol smooths fine lines. Glycolic acid smooths fine lines. Why not both? Because the mechanism of "smoothing" is essentially the same in both cases: increased cell turnover and removal of the upper, dead layers of the stratum corneum. AHAs do this by loosening the corneodesmosomes that hold dead skin cells together, while BHAs (salicylic acid) penetrate sebaceous follicles and exfoliate from within (Kornhauser et al., 2010). Retinoids do it by accelerating keratinocyte differentiation and turnover at the cellular level.
Stack them and you are essentially exfoliating your skin at twice the speed it can rebuild itself. The stratum corneum thins. Trans-epidermal water loss increases. Your skin becomes more reactive, redder, sometimes flaky. This is the textbook profile of compromised barrier function (Draelos, 2005).
Practical solution: alternate evenings. Retinol on Mon/Wed/Fri, AHA or BHA on Tue/Thu. Or rotate weekly. Skin needs recovery time between exfoliating actives.
3. Retinol + Benzoyl Peroxide (the acne overlap)
Both are acne fighters. Both are in almost every acne routine. But mixing them in the same step is a chemistry problem, not just an irritation problem. Classic retinoids like tretinoin are oxidatively degraded by benzoyl peroxide. The result: when you layer them, you are essentially deactivating your retinoid. Older clinical work showed up to 50% loss of tretinoin activity when applied with benzoyl peroxide (Nyirady et al., 2002).
The good news: newer retinoids like adapalene are photostable AND BPO-stable, which is why you see them combined into a single FDA-approved product (Epiduo / adapalene-BPO gel). If you are using over-the-counter retinol or prescription tretinoin alongside benzoyl peroxide, separate them into AM (BPO) and PM (retinoid). If you are using adapalene, layering is genuinely fine.
4. AHAs + BHAs together (acid stacking)
An AHA toner, then a BHA serum, then maybe an exfoliating mask "once a week"? That is acid on acid on acid. Each time you exfoliate aggressively, you remove some of the protective lipid matrix that holds your stratum corneum together. Done in moderation, this is fine. Done daily with stacked acids, you reach the over-exfoliation point fast, and the symptoms (stinging, shiny tight skin, paradoxical breakouts, redness) often get misread as "I need MORE actives" rather than "I need to stop."
Practical rule: pick the acid that targets your dominant concern (BHA for congestion and acne, AHA for texture and dullness) and use that two to three times a week. Do not use both on the same day.
5. Vitamin C (LAA) + AHAs / BHAs in the same step
Same logic as above: stacking acidic actives at the same step gives you no extra benefit and a lot of extra sting. If you really want to use vitamin C and an exfoliating acid in the same routine, apply the acid first, wait 15 to 20 minutes for skin pH to normalise, and then apply vitamin C. But honestly, vitamin C in AM and acid in PM is simpler, gentler, and just as effective.
6. Benzoyl Peroxide + AHA / BHA
Two oxidative/chemical exfoliating mechanisms colliding on the same skin. Benzoyl peroxide produces reactive oxygen species inside the follicle to kill Cutibacterium acnes. Salicylic acid simultaneously chemically exfoliates the follicle. Used together at strength, you get redness, peeling, and a measurable spike in post-inflammatory pigmentation, especially in skin of colour. Alternate them. Or pair BPO with niacinamide in one routine, and BHA with hydrators in the other.
7. The vitamin C + niacinamide "myth" (please stop worrying about this one)
I am including this one in the cannot-combine table specifically so I can debunk it. A 1960s in vitro study showed that ascorbic acid and niacinamide can form a 1:1 complex under high temperature and extreme pH conditions, producing a slight yellowing reaction. The internet ran with it for decades. Modern formulations at room temperature, at the pH levels found in actual skincare products, do not show this reaction in any meaningful way. A review by Wohlrab & Kreft (2014) explicitly addressed niacinamide's tolerability and compatibility, noting no meaningful clinical issue with combining it with other actives including vitamin C (DOI).
Vitamin C + niacinamide is, in fact, one of the smartest brightening combinations available.
The combinations you SHOULD use, sorted by skin goal
Now the fun part. Here are the combinations that are genuinely synergistic, organised by what you are actually trying to achieve.
Anti-ageing: the AM antioxidant shield + PM regeneration combo
The strongest evidence for an anti-ageing combination is the vitamin C + vitamin E + sunscreen trio in the morning. Vitamin C and vitamin E work synergistically: vitamin E neutralises lipid-soluble free radicals, gets oxidised in the process, and is then regenerated by vitamin C (Burke, 2007). Layered under sunscreen, this trio significantly reduces UV-induced erythema, DNA damage, and the matrix metalloproteinase activity that breaks down collagen.
In the evening, the smart pairing is retinol + peptides + ceramides. Retinol drives the cellular turnover and collagen signalling. Peptides are short amino-acid sequences that can either signal collagen production (matrikines like Matrixyl) or relax expression-line muscles (neuropeptides like Argireline) (Schagen, 2017). Ceramides reinforce the barrier, which is critical because retinol is mildly disruptive to barrier function during the early adjustment phase. Stack them and you get the active benefits of retinol with the structural support to tolerate it.
Hyperpigmentation: hit melanin from multiple angles, then block UV
Pigmentation is the goal where combination therapy genuinely outperforms monotherapy, because melanin synthesis is a multi-step process and you can target different steps with different ingredients. Vitamin C inhibits tyrosinase (the rate-limiting enzyme in melanin synthesis). Niacinamide blocks the transfer of melanosomes from melanocytes to keratinocytes, reducing pigment delivery to the upper skin (Hakozaki et al., 2002). Tranexamic acid interferes with the plasmin pathway involved in UV-stimulated melanogenesis and has shown strong clinical results in melasma (Kim et al., 2017). Azelaic acid is an additional tyrosinase inhibitor with anti-inflammatory properties, particularly useful for post-inflammatory hyperpigmentation.
And then sunscreen. Without it, none of the above will get you anywhere, because UV exposure constantly re-stimulates melanin production (see our sunscreen guide for what to look for). The takeaway: vitamin C + niacinamide + SPF in the morning, tranexamic or azelaic acid in the evening. Multi-pathway, gentle, synergistic.
Acne: layered, not stacked
Acne is the goal where people get into the most trouble with stacking, because there are SO many active options. The smart approach is to combine ingredients that hit different stages of acne pathogenesis (sebum, follicular keratinisation, C. acnes, inflammation) without compounding irritation.
A good evidence-based combination is BHA + niacinamide. Salicylic acid penetrates the sebaceous follicle and exfoliates the inside, addressing comedones at the source. Niacinamide reduces sebum production and inflammation, and supports the barrier (Wohlrab & Kreft, 2014). For more inflammatory acne, the fixed-combination prescription product adapalene + benzoyl peroxide is one of the most clinically validated acne treatments available (Gollnick et al., 2009). Adapalene is photostable AND BPO-stable, which is why this combination works in a single tube.
Azelaic acid deserves a special mention here. It is anti-inflammatory, antibacterial against C. acnes, mildly comedolytic, AND inhibits tyrosinase (which helps with the post-acne pigmentation that often becomes the bigger cosmetic problem after the active acne is gone). It plays well with almost every other active and is one of the most underused tools in mainstream skincare (Sieber & Hegel, 2014).
Sensitive / reactive skin: stop and rebuild first
If you are reading this with red, stinging, tight skin, you do not need MORE actives. You need to stop, repair, and start again with one ingredient at a time.
The barrier-rebuild combination is niacinamide + Centella asiatica + panthenol + ceramides. Niacinamide stimulates ceramide synthesis in the skin and reduces trans-epidermal water loss. Centella asiatica (and its bioactives madecassoside and asiaticoside) has been shown to support wound healing and reduce inflammation (Bylka et al., 2014). Panthenol (provitamin B5) is humectant and soothing. Ceramides are the lipid molecules that physically hold your skin barrier together; topically applied ceramides have measurable effects on barrier recovery (Loden, 2003). Use this combination AM and PM for two to four weeks before reintroducing any actives, one at a time, slowly.
Dehydrated skin: the layering hierarchy actually matters
Hyaluronic acid is the cornerstone humectant in skincare, attracting water into the upper layers of the skin. Glycerin is a smaller humectant that does the same thing at a different molecular weight. Ceramides and squalane act as occlusives that seal the moisture in. Apply humectants on damp skin (so they pull water from the moisture layer rather than from the deeper skin), then layer the occlusive on top to lock it in. This is one of the safest, most universally compatible combinations and works for every skin type alongside almost any active.
Acne scars (PIH): the lesson from the personal story
Going back to my friend's situation: she WAS, in principle, targeting the right thing. Vitamin C is great for fading post-inflammatory hyperpigmentation. Retinol is great for accelerating the turnover of pigmented cells and supporting collagen remodelling in atrophic scars. The combination of both is genuinely the gold-standard topical approach for acne scarring. Her mistake was layering them in the same routine. Once she split them (vitamin C in the AM with sunscreen, retinol in the PM, niacinamide in both routines), her skin calmed down within two weeks and she actually started seeing the brightening results she wanted.
The AM / PM cheat sheet
Most combination problems disappear if you split your actives across morning and evening intelligently. Here is a clean template you can build any routine on top of:
Notice how few actives are in there. That is the point. A working routine has one or two stars per session, not five. Everything else is supportive (hydration, barrier, sunscreen).
OK Emma great, now what's the actual takeaway?
Products worth trying
Some well-formulated picks, organised by skin goal.
Anti-ageing (Vitamin C AM / Retinol PM split)
Hyperpigmentation
Acne / congestion
Sensitive / barrier-rebuild
And the bigger lesson: if your friend showed looking like mine did, the answer is almost never "add another active." The answer is: simplify, repair, then re-introduce one thing at a time, with intention.
Welcome to Skinsights. I dive in the science behind skincare so you don't have to.
References
- Mukherjee, S. et al. (2006). Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clinical Interventions in Aging, 1(4), 327-348. DOI
- Pullar, J.M. et al. (2017). The Roles of Vitamin C in Skin Health. Nutrients, 9(8), 866. DOI
- Fitzpatrick, R.E. & Rostan, E.F. (2002). Double-blind, half-face study comparing topical vitamin C and vehicle for rejuvenation of photodamage. Dermatologic Surgery, 28(3), 231-236. DOI
- Kornhauser, A. et al. (2010). Applications of hydroxy acids: classification, mechanisms, and photoactivity. Clinical, Cosmetic and Investigational Dermatology, 3, 135-142. DOI
- Draelos, Z.D. (2005). Concepts in skin care maintenance. Journal of Cosmetic Dermatology, 4(2), 96-102. DOI
- Nyirady, J. et al. (2002). The stability of tretinoin in tretinoin gel microsphere 0.1%. Cutis, 70(5), 295-298. DOI
- Wohlrab, J. & Kreft, D. (2014). Niacinamide - mechanisms of action and its topical use in dermatology. Skin Research and Technology, 27(5), 311-315. DOI
- Burke, K.E. (2007). Interaction of vitamins C and E as better cosmeceuticals. Dermatologic Therapy, 20(5), 314-321. DOI
- Schagen, S.K. (2017). Topical Peptide Treatments with Effective Anti-Aging Results. Cosmetics, 4(2), 16. DOI
- Hakozaki, T. et al. (2002). The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. British Journal of Dermatology, 147(1), 20-31. DOI
- Kim, H.J. et al. (2017). Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Journal of the European Academy of Dermatology and Venereology, 31(11), 1777-1786. DOI
- Sieber, M.A. & Hegel, J.K.E. (2014). Azelaic acid: properties and mode of action. Skin Pharmacology and Physiology, 27 Suppl 1, 9-17. DOI
- Gollnick, H.P.M. et al. (2009). A randomized, single-blind, vehicle-controlled study to evaluate the efficacy and safety of adapalene-benzoyl peroxide combination gel in moderate to severe acne vulgaris. British Journal of Dermatology, 161(5), 1180-1189. DOI
- Bylka, W. et al. (2014). Centella asiatica in dermatology: an overview. Journal of Cosmetic Dermatology, 13(1), 32-37. DOI
- Loden, M. (2003). Role of topical emollients and moisturizers in the treatment of dry skin barrier disorders. American Journal of Clinical Dermatology, 4(11), 771-788. DOI