AHAs, BHAs and PHAs. Let's actually figure out which acid you need.


My personal story with acids
A few years ago, The Ordinary was everywhere on social media. The Glycolic Acid 7% Toning Solution, the AHA 30% + BHA 2% Peeling Solution (yes, the famous red one). It looked simple. It was cheap. And everyone on social media was swearing by it.
So I jumped in. I started using the glycolic toner basically every night. And then I added in the 30% peel a couple times a week, because it sounded extra effective. The first thing I noticed was the tingling. That sharp, slightly hot, "yep this is doing something" feeling. And I liked it. I thought: this is what working skincare feels like.
Then my skin got red. Then dry. Then patchy (especially around my eyes, even though I was not applying it there). By the time I realised something was wrong, my barrier was completely ruined. I had irritation bumps where I had never had a single spot before.
That tingling? That feeling I was loving? That was my skin literally telling me it was being damaged.
Tingling is not "working". It's irritation.
This is one of the biggest myths in skincare and it drives me a little bit crazy. People online keep promoting acids by saying things like "you'll feel it working" or "a little tingle means it's doing its job". That is just not true.
Properly formulated acids, at the right pH and the right concentration, should feel like almost nothing. Maybe a very slight warmth on the first few uses, and then nothing. If a product is stinging your face, your skin is signalling that the acid is too strong, the pH is too low, or your barrier is already compromised. None of those things are good.
That whole experience is actually the reason I went deep on the science of acids, especially for sensitive skin. Because I refused to believe that the only way to get the benefits (glow, smoother texture, fewer breakouts, less hyperpigmentation) was to burn your face off in the process.
Spoiler: it isn't. You just need to know what you're using and why.
What skincare acids actually do
Before we split them into families, let's talk about what they all have in common.
Your skin is constantly making new cells in the deep layer of the epidermis (the basal layer), and those cells slowly travel up to the surface, flatten out, and eventually shed off. That process is called desquamation. When you're young and healthy, it takes around 28 days. As you age, or if you have certain skin conditions, that process slows down. Dead cells stick around longer. Skin looks duller, feels rougher, pores look more visible, pigmentation lingers.
Skincare acids are chemical exfoliants. Instead of physically scrubbing dead cells off (which is mostly a bad idea), they loosen the "glue" that holds dead skin cells together so they shed more efficiently. That glue is mostly made of proteins called desmosomes and the cells around them. Acids interfere with those bonds.
The really important review by Kornhauser et al. (2010) in Clinical, Cosmetic and Investigational Dermatology walks through this beautifully. AHAs work by chelating (basically grabbing) calcium ions out of the desmosomes, which destabilises them. Less calcium, less adhesion, easier desquamation. BHAs and PHAs do something similar but with different chemistry and different reach into the skin. (DOI)
So all acids exfoliate. But they exfoliate differently, and that is what determines which one is right for you.
AHAs: surface renewal, glow and brightening
Alpha hydroxy acids are the family that includes glycolic acid, lactic acid, mandelic acid, malic acid, tartaric acid, and citric acid. They're called "alpha" because of where the hydroxyl group sits on the carbon chain. You do not need to memorise that.
The thing you do need to know: AHAs are water-soluble. That means they work on the surface of your skin and the upper layers of the stratum corneum, but they don't really go into your pores. They're surface-renewal acids.
How AHAs work
AHAs reduce calcium ions in the epidermis and disrupt corneocyte (dead skin cell) adhesion, so dead cells slough off faster (Kornhauser 2010). But that's just the start.
At higher concentrations and lower pH, AHAs (especially glycolic acid, which has the smallest molecule of the family) penetrate deeper and have effects in the dermis too. Bernstein et al. (2001) showed that twice-daily application of 20% glycolic acid for 3 months increased type I collagen mRNA and dermal hyaluronic acid in human skin. (DOI) Narda et al. (2021) confirmed that glycolic acid buffered to pH 4 stimulates collagen production and epidermal renewal in human skin explants, without triggering significant inflammation. (DOI)
That's why AHAs are not just "exfoliators". Used properly, they smooth fine lines, fade post-inflammatory hyperpigmentation, even out tone, and give that classic "glow" we all chase.
What AHAs are best for
AHAs shine for:
- Dullness and uneven texture. The surface renewal is what creates that fresh, reflective look.
- Hyperpigmentation and post-acne marks. Burns et al. (1997) showed that serial glycolic acid peels significantly improved post-inflammatory hyperpigmentation in patients with darker skin (Fitzpatrick IV-VI), with minimal side effects. (PubMed)
- Melasma, especially mandelic acid. Mandelic acid has a larger molecule than glycolic, so it penetrates more slowly and is better tolerated in pigmented skin. A comparative study by Garg et al. (2016) showed that a salicylic-mandelic peel was as effective as a 35% glycolic acid peel for active acne and post-acne hyperpigmentation, with better tolerability. (PubMed)
- Fine lines and early photoaging. Through that collagen mRNA stimulation we just talked about.
- Surface whiteheads (closed comedones near the surface). AHAs can help here because they renew the top layer where these sit. They do not reach deeper blackheads inside the pore.

Concentrations and how to build up
This is where most people mess it up. (Including past me.)
- Glycolic acid: Start at 5 to 7%, pH around 3.5 to 4. Use 2 to 3 nights a week for the first 2 to 4 weeks. Once your skin tolerates it, you can move to 8 to 10% and use every other night. Anything above 10% (peels, masks) is for occasional treatment use, not daily wear, and ideally not at home if you don't know what you're doing.
- Lactic acid: Gentler than glycolic because of its bigger molecule. Start at 5 to 10%. Great choice if your skin is on the drier side, since lactic acid also has humectant (water-binding) properties. Smith (1996) showed that lactic acid stimulates epidermal turnover in a pH-dependent way, so a pH around 3.5 to 4 is the sweet spot. (PubMed)
- Mandelic acid: The largest molecule in the AHA family, which means it penetrates the slowest and irritates the least. Start at 5 to 10%. This is the AHA I personally recommend for anyone with melanin-rich skin, hyperpigmentation, or sensitivity issues. You can use it 3 to 4 nights a week relatively early on.
The build-up rule I now live by: start low, stay there for at least 2 weeks, then increase frequency before you increase strength. Skin adapts. Rushing the process is what burnt my face the first time around.
Important note: AHAs do increase your skin's UV sensitivity. The FDA actually requires AHA products to carry a sunburn alert because studies showed that 4 weeks of AHA use roughly doubled UV-induced cellular damage. (FDA) Good news: the effect is reversible once you stop using them. The actual takeaway is just: SPF every single morning, no exceptions, especially while using AHAs.
BHAs: into the pore, for blackheads and oily skin
Beta hydroxy acids in skincare basically means one ingredient: salicylic acid. (Technically there are others, like betaine salicylate and willow bark extract, but salicylic acid is the gold standard.)
The defining feature of BHAs: they are oil-soluble. Which sounds like a small chemistry detail but it changes everything about what they can do.
How BHAs work
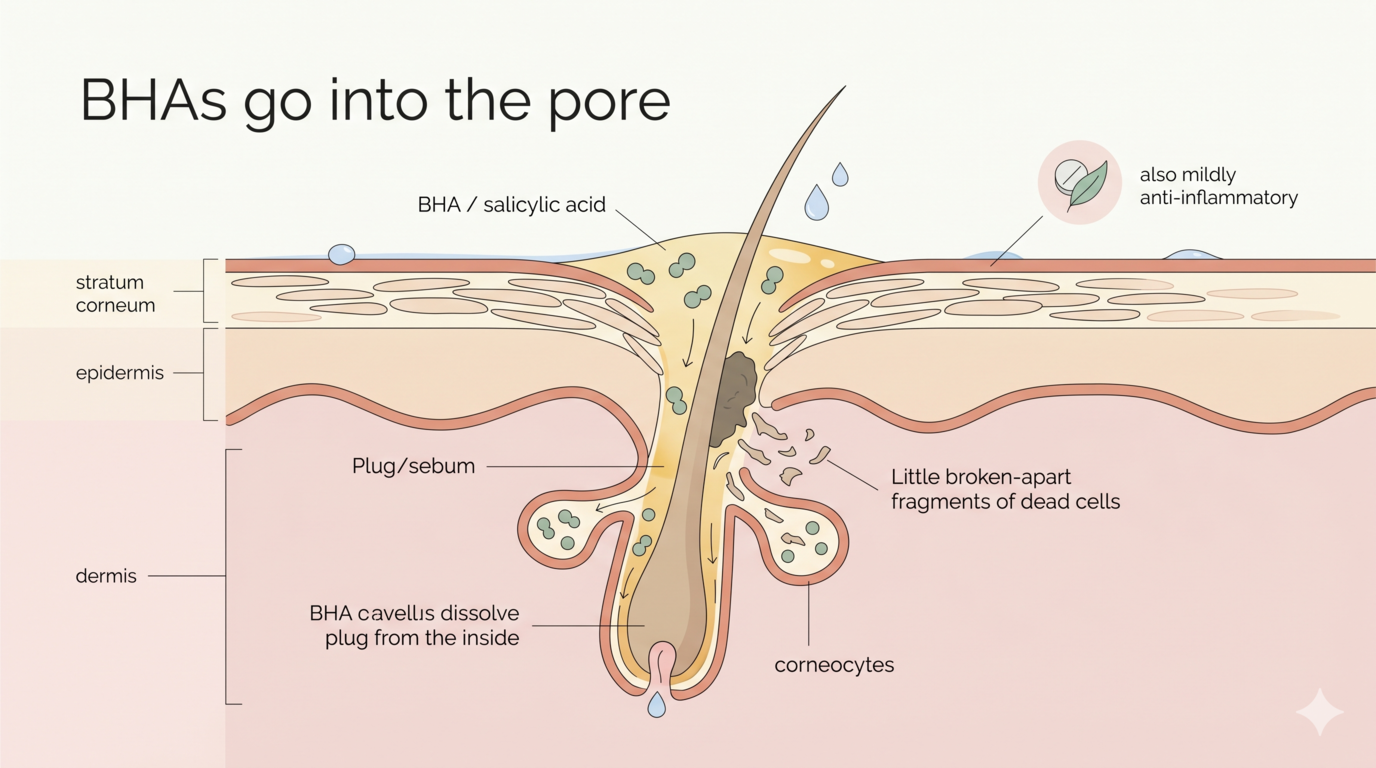
Because salicylic acid is lipophilic (oil-loving), it can dissolve into sebum and travel down into your pore lining. It doesn't just sit on the surface like AHAs. It actively goes into the follicle and breaks apart the cellular plug that creates blackheads and clogged pores.
The detailed review by Arif (2015) explains it really clearly: salicylic acid disrupts the desmosomes between corneocytes (so it exfoliates like AHAs do), but its lipid solubility means it concentrates inside sebaceous follicles, where comedonal acne actually starts. It's also a mild anti-inflammatory (chemically related to aspirin, which is why there is this DIY hack online of putting aspirine on your spots. Don't do this please, but use BHA instead), which calms inflamed acne lesions. (DOI)
So if AHAs are the surface-renewal acids, BHAs are the pore-clearing acids.
What BHAs are best for
- Blackheads and clogged pores. The lipid solubility is unique. AHAs do not do this.
- Oily and combination skin. Helps regulate the buildup that comes with higher sebum production.
- Acne, especially inflamed acne. Combines comedolytic action with anti-inflammatory effect.
- Acne-prone skin that also has redness. Surprising but well-documented. BHAs are often better tolerated than AHAs on inflamed skin because of that anti-inflammatory side.
- Sebaceous filaments (those tiny dots on your nose that aren't really blackheads). Won't make them disappear forever (they grow back, it's normal anatomy) but BHA keeps them less visible.
Concentrations and how to build up
- Salicylic acid for daily/regular use: 0.5 to 2% is the over-the-counter range and it's well-studied. Most leave-on serums and toners sit at 1 to 2%, pH around 3 to 4.
- Cleansers: 2% salicylic in a cleanser is gentler than in a leave-on, because the contact time is short. Good entry point if you're nervous.
- Higher % peels (10 to 30%): Professional treatment territory. Do not do this at home unless you really know what you're doing.
Build-up plan: start with a 1 to 2% leave-on product, 2 to 3 evenings a week. Once skin is happy (no flaking, no persistent redness), increase to every other night, or even nightly if your skin is oilier and tolerates it well. Most acne-prone skin can comfortably handle daily salicylic acid use long-term, which is one of the reasons it's such a workhorse.
Good news compared to AHAs: salicylic acid does not significantly increase UV sensitivity in the same way. But you still want SPF every day, because hello, sun damage is the number one driver of pigmentation and ageing regardless.
PHAs: the gentle resurfacers for sensitive skin
This is the family I wish I had known about when I was burning my face with The Ordinary peel.
Polyhydroxy acids include gluconolactone, lactobionic acid, and maltobionic acid. They're often called "next-generation AHAs" because they exfoliate similarly but in a gentler way.
How PHAs work
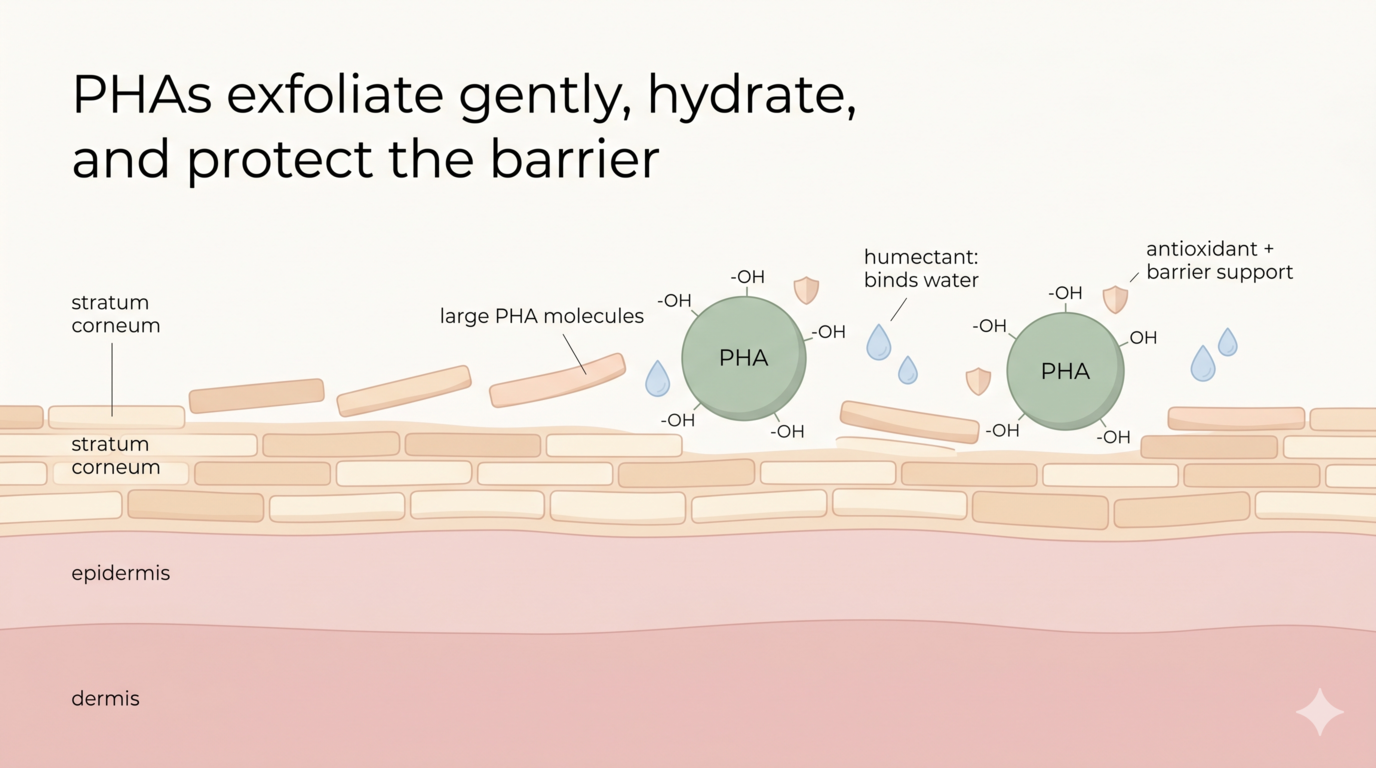
PHAs have a much larger molecular structure than AHAs (multiple hydroxyl groups, sometimes with a sugar attached). That bigger size means they cannot penetrate as deeply or as quickly. So they exfoliate primarily at the surface, very slowly, without the sting.
Grimes et al. (2004) published the landmark study in Cutis showing that a PHA-based regimen provided antiaging benefits comparable to a glycolic acid regimen over 12 weeks, but with significantly less irritation. (PubMed) Edison et al. (2004) confirmed in a separate split-face study that PHAs were equivalent to AHAs in efficacy for photoaged skin, but were better tolerated. (PubMed)
And here's where PHAs get really interesting. Because of all those hydroxyl groups on the molecule, PHAs do a few extra things that AHAs don't:
- They're humectants. They bind water to the skin while they exfoliate. So instead of leaving skin dry and tight, they leave it hydrated.
- They're antioxidant chelators. They bind metal ions that drive oxidative damage and inhibit matrix metalloproteinases (the enzymes that break down collagen). Algiert-Zielińska et al. (2018) describe lactobionic acid in particular as a strong antioxidant and barrier-supporting molecule. (PubMed)
- They actually support the skin barrier rather than weakening it. Which is why PHAs are safe for rosacea, atopic dermatitis, post-procedure skin, and sensitive skin types.
What PHAs are best for
- Sensitive skin and rosacea. Where AHAs sting and worsen redness, PHAs are usually tolerated.
- Compromised or recovering skin barriers. If you've over-exfoliated (hi, past me), PHAs are how you reintroduce chemical exfoliation safely.
- Post-acne marks on reactive skin. When mandelic or glycolic still feels too harsh.
- Mature or dry skin that wants exfoliation plus hydration.
- People who are using other actives (retinol, vitamin C) and want a low-conflict exfoliant. PHAs play very nicely with everything else.
Concentrations and how to build up
- Gluconolactone: Common at 4 to 10% in leave-on products. Even 10% is well-tolerated by most sensitive skin.
- Lactobionic acid: Often formulated at 5 to 10%, sometimes higher in peels. Particularly good if your barrier is fragile.
Build-up is simpler with PHAs because the irritation risk is lower. You can usually start at every other evening and move to daily within 2 weeks. Many people with truly sensitive skin use PHAs as their only chemical exfoliant long-term, and that's a totally valid routine.
The one rule that applies to all acids
Sunscreen. Every. Morning. SPF 30 minimum, broad spectrum, regardless of which acid you're using.
Even with PHAs, where photosensitisation is minimal, you are still increasing cell turnover and exposing newer skin to UV. And UV is the single biggest driver of pigmentation, collagen breakdown, and uneven tone. There is no point doing the acid work if you don't protect the result. (If you want the deep dive on filters and SPF, see my sunscreen post.)
Are you already using other active ingredients (vitamin C, retinol, niacinamide,...)? Then check out my previous blogpost on which combination can be made, and which can't first.
OK Emma great, now which acid do I actually use?
Here is the cheat sheet. Find your skin and your goal, pick your acid.
A few product ideas, if you want a starting point
I'll keep this short because the actual ingredient matters more than the brand. But these are formulations I think are well-balanced and reasonably accessible. Always patch-test first.
- For AHA glow (glycolic): Pixi Glow Tonic (5% glycolic, well-buffered pH, very gentle entry point), or The Ordinary Glycolic Acid 7% if your barrier is healthy and you've used acids before.
- For AHA on dry skin (lactic): The Inkey List Lactic Acid 10% Serum, or Sunday Riley Good Genes (more expensive, but a beautifully formulated lactic acid).
- For AHA on pigmentation (mandelic): By Wishtrend Mandelic Acid 5% Skin Prep Water, or The Ordinary Mandelic Acid 10% + HA.
- For BHA (salicylic): Paula's Choice 2% BHA Liquid Exfoliant is the most studied OTC formulation around. CeraVe SA Cleanser is a softer cleanser option.
- For PHA (sensitive skin and barrier repair): NeoStrata PHA Facial Cleanser, Inkey List PHA Toner, or Stratia Soft Touch AHA (which actually combines low-% AHA with PHAs and is very gentle).
Some last takeaways
Acids work. The science is solid. They renew skin, fade pigmentation, clear pores, and support collagen. But the "more is better" mindset will wreck your skin (it wrecked mine). The right acid for you depends entirely on your skin type, your barrier status, and your goal. Not on what's trending.
Three things to remember:
- Tingling and stinging are not signs that an acid is "working". They're signs of irritation. Good acid use should feel like almost nothing.
- Pick by mechanism, not marketing. AHAs for surface and tone, BHAs for pores and oil, PHAs for sensitive skin and barrier-friendly exfoliation.
- Start low, go slow, and always wear SPF. Your future skin will thank you.
Welcome to Skinsights. I dive in the science behind skincare so you don't have to.
Scientific References
- Kornhauser A, Coelho SG, Hearing VJ. "Applications of hydroxy acids: classification, mechanisms, and photoactivity." Clin Cosmet Investig Dermatol. 2010;3:135-142. DOI
- Bernstein EF, Lee J, Brown DB, Yu R, Van Scott E. "Glycolic acid treatment increases type I collagen mRNA and hyaluronic acid content of human skin." Dermatol Surg. 2001;27(5):429-433. DOI
- Narda M, Brown A, Muscatelli-Groux B, Grimaud JA, Granger C. "Glycolic acid adjusted to pH 4 stimulates collagen production and epidermal renewal without affecting levels of proinflammatory TNF-alpha in human skin explants." J Cosmet Dermatol. 2021;20(2):513-521. DOI
- Smith WP. "The roles of pH and concentration in lactic acid-induced stimulation of epidermal turnover." Dermatol Surg. 1996;22(8):709-713. PubMed
- Burns RL, Prevost-Blank PL, Lawry MA, Lawry TB, Faria DT, Fivenson DP. "Glycolic acid peels for postinflammatory hyperpigmentation in black patients. A comparative study." Dermatol Surg. 1997;23(3):171-174. PubMed
- Garg VK, Sinha S, Sarkar R. "Comparative Evaluation of Efficacy and Tolerability of Glycolic Acid, Salicylic Mandelic Acid, and Phytic Acid Combination Peels in Melasma." Dermatol Surg. 2016;42(3):384-391. PubMed
- Arif T. "Salicylic acid as a peeling agent: a comprehensive review." Clin Cosmet Investig Dermatol. 2015;8:455-461. DOI
- Grimes PE, Green BA, Wildnauer RH, Edison BL. "The use of polyhydroxy acids (PHAs) in photoaged skin." Cutis. 2004;73(2 Suppl):3-13. PubMed
- Edison BL, Green BA, Wildnauer RH, Sigler ML. "A polyhydroxy acid skin care regimen provides antiaging effects comparable to an alpha-hydroxyacid regimen." Cutis. 2004;73(2 Suppl):14-17. PubMed
- Green BA, Yu RJ, Van Scott EJ. "Clinical and cosmeceutical uses of hydroxyacids." Clin Dermatol. 2009;27(5):495-501. DOI
- Algiert-Zielińska B, Mucha P, Rotsztejn H. "Lactic and lactobionic acids as typically moisturizing compounds." Int J Dermatol. 2019;58(3):374-379. PubMed
- Draelos ZD, Green BA, Edison BL. "An evaluation of a polyhydroxy acid skin care regimen in combination with azelaic acid 15% gel in rosacea patients." J Cosmet Dermatol. 2006;5(1):23-29. DOI
- U.S. Food and Drug Administration. "Alpha Hydroxy Acids." Cosmetic Ingredients Information. FDA